Table of Contents >> Show >> Hide
- What “Botox for Sweating” Actually Means
- How Botox Stops Sweat (Without Turning You Into a Desert)
- Who’s a Good Candidate (and Who Needs a Work-Up First)
- Targeted Areas: Where Botox Is Used for Excessive Sweating
- What the Appointment Is Like (Step-by-Step, Minus the Drama)
- When It Kicks In and How Long It Lasts
- Cost: What Botox for Sweating Usually Runs (and Why the Price Jumps Around)
- Effectiveness: What Results Can You Realistically Expect?
- Risks and Side Effects (The Honest List)
- Aftercare: How to Get the Best Results (and Avoid Dumb Problems)
- Botox vs. Other Hyperhidrosis Treatments: Where It Fits
- Quick FAQs
- Experiences: What People Commonly Notice (The 500-Word Reality Check)
- Conclusion
If your sweat glands behave like they’re paid by commissionsoaking shirts, sabotaging handshakes, and turning “just nervous” into “did you run here?”you’re not alone. Excessive sweating (hyperhidrosis) is common, frustrating, and wildly good at showing up at the worst possible moments.
Enter: Botox. Yes, the same injectable famous for smoothing wrinkles also has a very practical side hustlereducing sweat. And unlike that “clinical-strength” antiperspirant you’ve been rage-applying like frosting, Botox works by interrupting the signal that tells sweat glands to go full fire-hydrant.
In this guide, we’ll break down how Botox for sweating works, where it’s used, how much it typically costs, how long it lasts, what the appointment is like, and the real risks (including the rare but serious ones). We’ll also end with a 500-word “what people experience” section so you know what to expect beyond the brochure.
What “Botox for Sweating” Actually Means
Botox is a brand name for onabotulinumtoxinA, a purified protein that temporarily blocks certain nerve signals. For sweating, it’s used to treat primary focal hyperhidrosismeaning heavy sweating that’s not caused by another medical condition and usually affects specific areas like the underarms, palms, soles, scalp, or face.
In the United States, Botox is FDA-approved for severe primary axillary hyperhidrosis (translation: serious underarm sweating) when topical agents haven’t been enough. Use in other body areas is common in clinical practice, but those uses are typically considered off-label, meaning the doctor may use it based on evidence and experience even if it’s not the exact FDA-approved indication.
How Botox Stops Sweat (Without Turning You Into a Desert)
Sweating is controlled by nerves that release a chemical messenger called acetylcholine. That messenger is basically the “Go!” button for your eccrine sweat glands.
Botox works by blocking the release of acetylcholine at the nerve endings near the sweat glands. No acetylcholine signal, no overachieving sweat response. The glands don’t get removed or “killed”they just stop receiving the spammy “SWEAT NOW!!!” notifications for a while.
The result is localized sweat reduction in the treated area. You still sweat elsewhere (and you still need it to regulate body temperature). Botox isn’t an “anti-sweat spell” for your whole bodyit’s targeted, by design.
Who’s a Good Candidate (and Who Needs a Work-Up First)
Botox is usually considered when excessive sweating:
- Is focal (underarms, hands, feet, scalp, face, etc.),
- Is predictable and disruptive (work, social life, clothes, tools, sports),
- Hasn’t responded well to topical antiperspirants or prescription-strength options, and
- Is consistent with primary hyperhidrosis rather than a symptom of another condition.
Before treating sweating “symptom-first,” clinicians commonly check for signs of secondary hyperhidrosissweating driven by something else (thyroid disease, diabetes, infections, menopause, medication side effects, and more). If there’s a treatable cause, it’s smarter to treat that rather than just muting the sweat alarm. (In other words: don’t put duct tape over the check-engine light.)
Practical tip: Bring notes. When does sweating happenday, night, during sleep, with stress, with heat? Which areas? Any new meds? Patterns matter for diagnosis and insurance coverage.
Targeted Areas: Where Botox Is Used for Excessive Sweating
Botox can be used in several sweat-prone zones. Here’s the reality-based breakdown:
Underarms (Axillary Hyperhidrosis)
This is the most common, most studied, and FDA-approved area. Underarm treatment tends to be straightforward, relatively tolerable, and highly effective for many patients.
Hands (Palmar Hyperhidrosis)
Dermatologists often treat sweaty palms with Botox, especially when hand sweating affects work (healthcare, service jobs, tech, crafts) or quality of life. The catch: injections can be more uncomfortable, and temporary hand muscle weakness can happen, which matters if you rely on grip strength or fine motor work.
Feet (Plantar Hyperhidrosis)
Botox may help sweaty feet, but the soles can be sensitive and treatment can be painful without strong numbing strategies. Results may not last as long as underarms for some people, and you still need to consider shoe/skin care to prevent odor and irritation.
Face/Scalp
Some clinicians treat forehead sweating or scalp sweating (the kind that makes your hair look like it just finished a marathon). Facial anatomy is more delicateplacement and dosing matter to avoid issues like eyelid droop. This is one of those “choose your clinician carefully” zones.
Other Areas (Groin, Under-Breast, Back, Etc.)
Yes, sweating can happen there, and yes, some clinicians treat it. But these areas are more individualized in technique and may have less standardized evidence than underarms. Expect a more customized planand a longer conversation about risks, cost, and realistic goals.
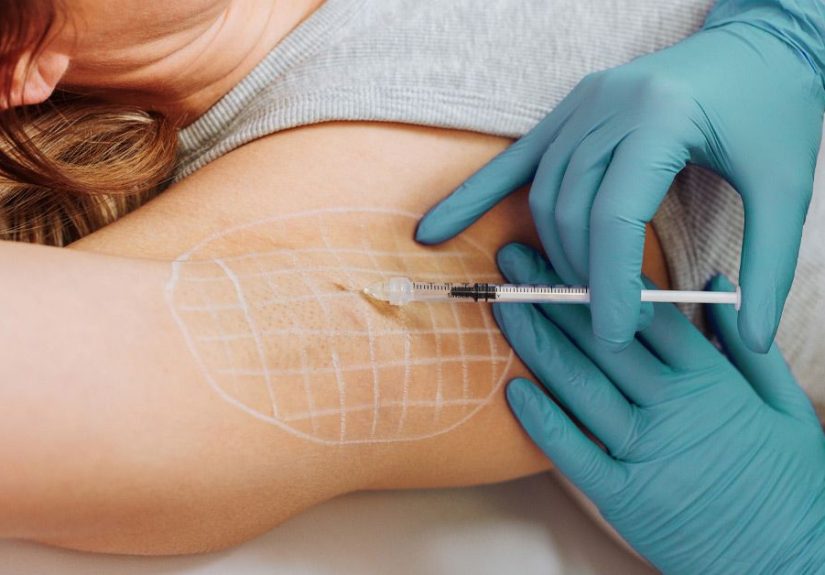
What the Appointment Is Like (Step-by-Step, Minus the Drama)
1) Mapping the Sweat Zone
For underarms, clinicians often use a mapping method such as the iodine-starch test (often called Minor’s test), which helps highlight the most active sweating areas so injections can be placed evenly and efficiently.
2) Numbing (Optional but Popular)
Underarms: many people do fine with ice or topical numbing cream. Hands/feet: numbing becomes a bigger dealsome practices use nerve blocks or stronger local anesthesia strategies.
3) The Injections
Underarm Botox is injected intradermally (just under the skin surface) in multiple small spots. A typical pattern uses about 10–15 injection sites per underarm, spaced roughly 1–2 cm apart.
For FDA-approved underarm treatment, the commonly referenced dose is 50 units per axilla (100 units total), distributed across those sites. The needle is small (often 30-gauge), and the whole thing is usually done in minutes, not hours.
4) Back to Life
Most people go right back to work the same day. You might be slightly tender or bruised, but you’re not typically “down for the count.” Think: mild inconvenience, not dramatic recovery montage.
When It Kicks In and How Long It Lasts
Botox isn’t instant. Many people notice improvement within about a week, with full effect often showing up over 1–2 weeks. Duration varies by area and individual, but underarm results commonly last for several months.
Real-world ranges reported by dermatology sources often look like this:
- Underarms: often around 3–10 months for many patients
- Hands: often a similar multi-month window, but can vary
- Feet: sometimes shorter for some patients
- Face: often several months
Repeat treatments are typically done when the effect fades and symptoms returnnot on a rigid calendar. Some people come back twice a year; others stretch longer.
Cost: What Botox for Sweating Usually Runs (and Why the Price Jumps Around)
Botox pricing is famously variable, because it depends on:
- How many units are used (more area = more units),
- Whether pricing is per unit or per area (or both),
- Clinician expertise and regional costs,
- Facility fees, and
- Whether insurance helps.
Typical Out-of-Pocket Ballpark
For underarms, a commonly quoted out-of-pocket total is around $1,000 for both underarms in many U.S. clinics, though it can be higher or lower depending on your market and provider.
Hands and feet can cost more because they often require more units, more time, and sometimes additional anesthesia. If you’re treating multiple areas (say, underarms plus palms), costs can stack quickly.
Can Insurance Cover It?
Sometimesespecially for severe primary axillary hyperhidrosis with documentation that topical treatments weren’t enough. Coverage varies by plan and usually involves prior authorization. Translation: you may need your clinician to submit notes, severity scoring, treatment history, and sometimes proof that prescription antiperspirants or other therapies were tried first.
Coverage is less consistent for off-label areas (like palms, soles, scalp), but some insurers do approve in specific cases. If cost is your biggest barrier, ask your clinic what documentation they use and whether they have staff who handle hyperhidrosis authorizations.
Effectiveness: What Results Can You Realistically Expect?
For severe underarm hyperhidrosis, clinical studies and clinical practice both support substantial sweat reduction in many patients. In FDA labeling studies for axillary hyperhidrosis, response rates favored Botox significantly compared with placebo.
The most satisfying outcome is not always “zero sweat forever.” Often it’s:
- Shirts survive the day without visible sweat marks,
- Hands stop slipping on pens, tools, steering wheels, and phones,
- Foot odor and dampness ease up,
- Confidence returns because you’re not planning outfits like you’re preparing for a rainfall.
If you’re expecting Botox to make your skin feel like a desert planet 24/7, that’s usually not the goal. Most people want “normal-human sweating,” not “museum artifact preservation.”
Risks and Side Effects (The Honest List)
Any injection-based treatment has potential downsides, even when it’s routine. Most side effects are mild and temporary, but there are also rare serious risks.
Common, Usually Mild Side Effects
- Injection site pain, tenderness, swelling, bruising, or minor bleeding
- Headache or feeling “flu-ish” for a short period
- Sore throat or mild upper respiratory symptoms reported in some patients
- Dryness in the treated area (sometimes welcomed, sometimes annoying)
- Non-treated-area sweating may occur in some patients (not everyone experiences this)
Area-Specific Risks
- Hands: temporary weakness in grip or fine motor function can happen (important for musicians, surgeons, climbers, mechanics)
- Face: drooping eyelid (ptosis) is a known risk if toxin affects nearby muscles
- Feet: treatment can be painful; soreness may affect walking briefly
Rare but Serious: Spread of Toxin Effects
Botox carries a warning that effects can, in rare cases, spread beyond the injection site and cause symptoms consistent with botulinum toxin effects. These can include generalized muscle weakness, trouble swallowing, trouble speaking, or breathing difficulties. While this is uncommonespecially at typical hyperhidrosis dosingit’s serious enough that you should know the warning signs and seek urgent care if they occur.
Who Should Use Extra Caution?
Tell your clinician if you have a neuromuscular disorder, prior issues with swallowing/breathing, or take medications that can affect neuromuscular transmission (certain antibiotics or muscle relaxants). Also discuss pregnancy or breastfeedingrisk/benefit decisions should be individualized.
Aftercare: How to Get the Best Results (and Avoid Dumb Problems)
- Don’t scrub the area aggressively the same day. Be nice to your skin.
- Avoid intense heat or heavy workouts for the rest of the day if your clinician advises it (some practices recommend keeping it chill for 24 hours).
- Skip antiperspirant for a short window if instructed, especially if you had a mapping test or irritation.
- Track your results around day 7–14 so you can report back accurately (helpful if dose/placement needs tweaking next time).
- Call your clinician if you have unusual weakness, difficulty swallowing, breathing problems, or severe symptoms.
Botox vs. Other Hyperhidrosis Treatments: Where It Fits
Botox is one strong optionoften a “middle path” between topical treatments and more permanent procedures. Depending on the area and severity, clinicians may also recommend:
- Clinical-strength and prescription antiperspirants (often aluminum chloride-based)
- Prescription topical anticholinergics for underarms
- Oral medications (anticholinergics) for more generalized controleffective for some, but side effects can be limiting
- Iontophoresis (especially for hands/feet)
- Microwave thermolysis for underarms (a more durable approach for some patients)
- Surgery (like sympathectomy) in select cases, balancing benefits with risks such as compensatory sweating
A good clinician will help you choose based on the “big three”: area, severity, and what you’ve already tried.
Quick FAQs
Will Botox stop sweating completely?
Some people get near-total dryness in the treated area; others get a strong reduction but still sweat a bit. Most people aim for “socially normal” sweating rather than “never again.”
Does it help with sweating at night?
Night sweats can suggest secondary causes. If sweating is generalized or happens during sleep, talk with a clinician before assuming it’s primary hyperhidrosis.
Will I smell worse if I sweat less?
Often the opposite. Sweat itself is odorless; smell tends to come from bacteria breaking down sweat on the skin. Less sweat can mean fewer “materials” for odor to developthough hygiene still matters.
How often will I need it?
Many people repeat treatment when symptoms return, often every few months. Your “refresh” schedule depends on how long your results last.
Experiences: What People Commonly Notice (The 500-Word Reality Check)
Let’s talk about the part most brochures skip: what it feels like to actually live with Botox for sweatingweek by week, shirt by shirt. People’s experiences vary, but there are patterns that show up often enough to be genuinely useful.
Right after treatment, underarms tend to be the easiest. People commonly describe it as “a bunch of quick pinches” and then it’s over. Some feel mild soreness or see tiny bruises that fade in a few days. Most go back to work immediatelythough a few prefer not to wear a tight white T-shirt the same day, because life is short and you don’t need to star in a “spot the bruise” game.
Days 3–7 are when many start playing the “Is it working or am I imagining things?” game. A common story: someone notices their usual “midday underarm check” suddenly feels… anticlimactic. Shirts stay drier, and the urge to pack backup clothes fades.
By week 2, the effect often feels more obvious. People report choosing colors they avoided before (hello, light gray), raising their arms without anxiety, and using less antiperspirant. One practical surprise is that some people need to rethink their deodorant routine: when you’re not sweating as much, heavy antiperspirant can feel sticky or irritating, so many switch to a gentler deodorant or use product less frequently.
Palms and soles are the “worth it, but plan ahead” areas. People who treat palms often say the discomfort is higher than underarms, but the benefit can be hugeespecially if hand sweating affects work, dating, gaming, musical performance, or literally holding a steering wheel. The most common tradeoff that gets mentioned is temporary grip weakness. For most, it’s mild, but if you depend on maximal hand strength, it’s something to discuss before treatment. People who treat feet often describe post-treatment soreness (the soles are sensitive!) and sometimes plan treatments before a quieter week rather than right before a big trip with 25,000 steps per day.
The cost experience is its own emotional journey. Out-of-pocket patients often describe it as an “investment in sanity” when it works well, but nobody loves paying for repeat sessions. Those who get insurance coverage usually say the paperwork is the hardest part: documenting failed topicals, severity, and quality-of-life impact. A helpful strategy many clinics suggest is keeping a short log (how many shirts ruined per week, work impacts, rashes, social avoidance) so the medical necessity story is clear and consistent.
When it wears off, it’s rarely dramatic. People usually notice sweat creeping back gradually over weeks. Many book their next session when they’re “80% back to old sweating” rather than waiting until it’s fully miserablebecause the goal is to stay ahead of the problem, not re-live it.
Bottom line: for the right person, Botox isn’t just “less sweat.” It’s fewer wardrobe calculations, fewer awkward moments, and a little more freedom to exist in public without thinking about armpits, palms, or socks every five minutes.
Conclusion
Botox for sweating is one of the more practical “modern medicine flexes”: a targeted treatment that can significantly reduce excessive sweating for months at a timeespecially in the underarms, where it’s FDA-approved. It’s not the cheapest option, and it’s not risk-free, but for many people, the payoff is huge: fewer sweat stains, fewer social worries, and a better quality of life.
If you’re considering treatment, the best next step is a consultation with a dermatologist or experienced clinician who treats hyperhidrosis regularly. A good plan will confirm whether your sweating is primary or secondary, set realistic expectations, and help you navigate cost and coverage.






